

As the COVID-19 pandemic of February and March 2020 unfolded like the slow-motion train wreck that it was and still is, each week brought a new, unexpected scene. For several weeks, we shopped for our groceries as we always had, but walked past shelves denuded of toilet paper, Clorox wipes and Purell. Politicians from the left urged us on TV to walk around in Chinese communities unprotected during their New Year celebration. As happened frequently to progressives, they dropped the ball with respect to pandemic control because they thought inclusiveness or racial justice were more important objectives than people getting sick and dying.
Nancy Pelosi encouraging people to visit Chinatown in San Francisco.
Governor Whitmer locking down Michigan and requiring face masks.
The Surgeon General of the United States went on Fox News and declared that face masks do not work https://www.foxnews.com/media/surgeon-general-explains-masks-public-coronavirus.
A few weeks later politicians were ordering the public to lock ourselves down in our homes and many governors ordered their constituents to wear masks in public. Again, they did so with such casual disregard for the economic consequences of that action it became difficult to understand if they had any priority than to issue orders and see that they were obeyed. That week, we began walking past the same supermarket shelves masked up like we were all planning to rob the store, as toilet paper made its return and then meat disappeared. Mask advocates invoked “the science” as if there was something obvious in the peer reviewed literature that formed the basis of this policy. There isn’t. There have been hundreds of studies of the patient risks during masked or unmasked medical procedures. There are no studies whatsoever as to the health outcomes of ordinary citizens wearing surgical masks as protective devices in a pandemic.
The use of the word “Mask” is an over simplification, because this controversy is really about three different things, each of them being separately defined and regulated as medical devices. A surgical mask is a disposable fabric filter designed to provide a protective barrier preventing the breath aerosols and droplets of the wearer from falling into a sterile surgical field. An N95 mask is a polymer enhanced version of the surgical mask that has been tested to retain 95% of particles of 0.3 microns diameter or more, and is more commonly called a dust mask, because they have found widespread use in the farming and construction industry to protect the wearer not from pathogens, but from inhalation of dusts, spores, and silica particles. The third device is a respirator, or a “rebreather” and this is a fully contained breathing system that allows the user to be enclosed in an impermeable suit with a mechanically driven HEPA filter cleaning all airborne particles and infectious agents from the breathable airstream. We currently have a controversial situation because health authorities have been requiring the population to employ device one, the surgical mask, as if it were a full respirator.
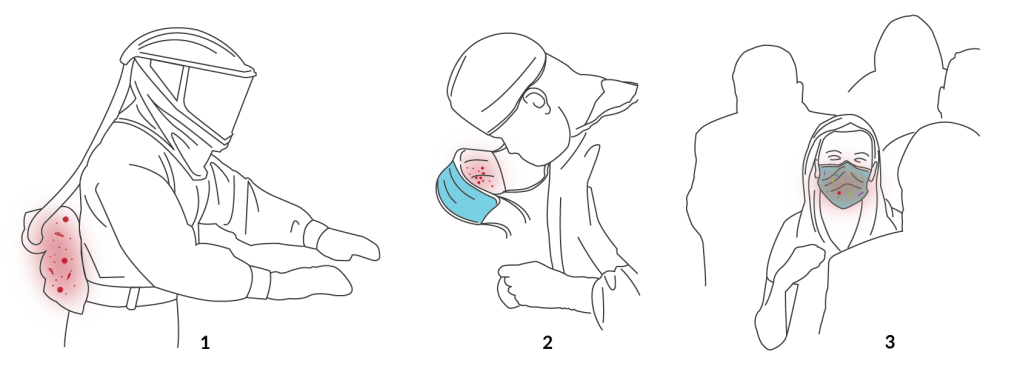
It’s informative to review the history of the first known COVID-19 patient identified in the United States, a 35 year old man who traveled directly from Wuhan, China in mid-January and presented in an emergency room in Washington on January 19, 2020. Quoting from the Bloomberg news article about his diagnosis,
“The test came back positive that afternoon, Jan. 20, the first confirmed case in the U.S. By 11:00 p.m., the patient was in a plastic-enclosed isolation gurney on his way to a bio-containment ward at Providence Regional Medical Center in Everett, Washington, a two-bed unit developed for the Ebola virus. As his condition worsened, then improved over the next several days, staff wore protective garb that included helmets and face masks. Few even entered the room; a robot equipped with a stethoscope took vitals and had a video screen for doctors to talk to him from afar.”
It is clear from this account the medical staff in Everett understood that if they were to protect themselves from respiratory particles coming from a COVID-19 patient, full-containment respiratory self-breathing suits were required. They had them and they wore them. A simple surgical mask was not going to cut it. American health authorities fully understood that respirators were critical to protect medical staff. But the few in stock around the nation were simply for theater, something cool to flash for CNN during their coverage of Ebola outbreaks. They were not even a miniscule fraction of the number required to manage a pandemic. So when this one arrived, medical workers were forced to rely on the N95 and procedure masks, already well established to be inadequate for their protection. History would bear witness to this inadequacy, as more than 100 Italian doctors not only contracted COVID-19 but also died of it. There are only 336,000 doctors in all of Italy, so using a case fatality rate of 1%, fully 10,000 physicians or 3% of all Italian doctors became infected because inadequate masks were included as PPE.
By requiring persons in states or countries under lockdown to wear surgical masks in public, health authorities have pushed the device beyond its design specifications. When used for hours by a wearer traversing crowded public spaces, the mask becomes akin to a collection device for sampling all available environmental pathogens. Respiratory droplets from dozens of people containing a variety of bacterial and viral pathogens are collected and retained a few mm from the lips and nose of the wearer, and maintained in a moist environment that enhances pathogen survival. Remember, a surgical mask is designed for the wearer to stand virtually immobile in an operating room environment, to wear the mask for a few hours at most, and to dispose of it antiseptically as if it were highly contagious. Current lockdown policies require users to wear this device while they traverse public spaces, intersecting the exhaled breath paths of numerous strangers. Because of the scarcity of masks, most of the general public do not dispose of their masks regularly or at all, but wear them repeatedly. A review of laboratory acquired infections over the past eighty years has shown that a self-contained rebreathing device is necessary to prevent the wearer from inhaling aerosolized live pathogens. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2493080/ and https://cmr.asm.org/content/cmr/8/3/389.full.pdf. The extreme cost, lack of availability, and cumbersome nature of this equipment that would have been necessary and sufficient to protect both emergency hospital workers and the general public from infection with SARS-CoV-2 is what led to the politically establishment of surgical mask misuse.
This situation has let to massively conflicting information about the use and effectiveness of surgical masks in public. Comments seen on Twitter include, “If masks work, then why don’t they just give all the prisoners masks instead of letting them out of jail? If masks work, then why do we have to stand 6 feet apart? If standing 6 feet apart works, then why do we need to wear masks?” Social media contributed further confusion as well by the creation of outright falsehoods masquerading, again, as science. Here’s one example:
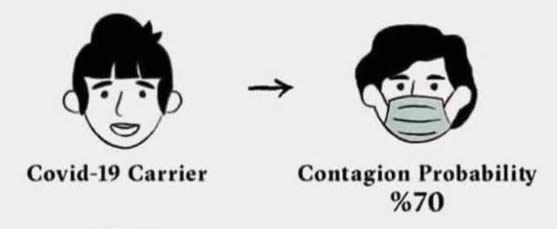
There is no scientific study to document this. A designed study of this type is unethical. Accidental exposures of this type can be studied. A study of the COVID-19 seroprevalence in NYC health care workers suggests that the true contagion probability is 1 or 2% even after repeated exposures. Only 7% of NYC health care workers had seroconverted or caught the illness even after weeks of repeated, daily exposures of this type. https://www.forbes.com/sites/lisettevoytko/2020/05/07/fewer-ny-healthcare-workers-are-being-infected-with-covid-19-compared-to-public-cuomo-says/#193104176619
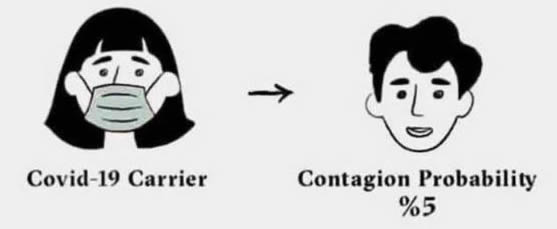
There is no scientific study to document this. Exposing any healthy subject to a COVID-19 positive patient, whether masked or not, is unethical. Instances where a completely unprotected health worker was exposed to a masked COVID-19 patient would be too rare to be meaningful.
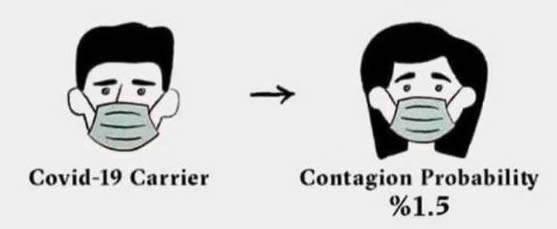
There is no scientific study to document this. It is possible that in a jurisdiction where all EMTs apply PPE to suspected COVID-19 patients before delivering them to PPE-protected health service providers in hospitals, and those providers never are exposed to any other source of the virus, one could derive a statistic. The scenario is improbable.
And finally, there is the homemade cloth version of a surgical mask. Many masks are homemade cotton cloth improvisations that filter droplets less well than polymer fiber masks, and retain more moisture. The inferiority of cloth masks to standard medical masks has been documented. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4420971/ Since there is clear scientific evidence that cloth masks have a negative impact on the spread of disease and the health of the user, public health authorities ought to be forbidding their use. Instead, the industriousness and creativity of cloth mask wearers are extolled, and they are made out to be heroes of the revolution.
At this point in the pandemic, the face mask has transcended it’s potential medical function and has become a simple political statement. 99.99% of mask wearers are healthy. The only impact the mask can have on their health is to catch and sequester a pathogen near their mucous membranes. Yet the mask is now a political symbol of subservience to authority and of polite contrition in the face of incomprehensible mandates by those paid to provide guidance. Masks are going to be with us for a long time. Upon reflection, we should have known that the face mask was doomed to become another piece of political theater. (See also, the TSA and political theater masquerading in place of substantive policy. https://kirkmaxey.com/2014/11/07/the-black-curtain-of-death-theatre-in-lieu-of-substance/ ) They have no cost to politicians, require no taxes or employees, and give a dramatic visual impression that something is being done. No amount of good science will be able to dislodge them now.
Fortunately, it is now summer where I live, and whenever I’m not wearing my mask, I can flip it up on the dashboard where the temperature is often 140 degrees fahrenheit under direct sunlight. Studies have shown that corona viruses and almost all respiratory viruses cannot survive more than a few minutes under these conditions.

There will never be an actual end to this pandemic, unless you define that as some time in the future when SARS-CoV-2 does not kill any substantial fraction of the people catching a seasonal respiratory virus. Considering the many unusual cardiovascular and immune aspects of corona virus, I think that day will be a long time coming. In the words of T.S. Eliot, it will die not with a bang but with a whimper. Even with an effective vaccine, life will not be without risk. It never has been. At some point, you just have to take that diaper off your face and get back to living.
